A Little Aviation Physiology
Anyone who flies, even as a passenger, can benefit from a basic knowledge of aviation physiology. It can be life-saving, as I hope to show. A detailed topic, but I will try to keep it short, sweet and practical. For those who want more details, a simple Google or Wikipedia search on the specific topic will provide it.
Understand that the usual study of physiology concerns itself with abnormal physiology in a “normal” environment. Aviation physiology is about normal physiology in an “abnormal” environment. In order to understand it, we need to understand that environment, i.e. the atmosphere.
Understand that the usual study of physiology concerns itself with abnormal physiology in a “normal” environment. Aviation physiology is about normal physiology in an “abnormal” environment. In order to understand it, we need to understand that environment, i.e. the atmosphere.
Physics of the Atmosphere

Most flight takes place in 3 layers or “strata” of the earth’s atmosphere. The Troposhere extends from the surface of the earth to about 35000 feet over the poles, and 65000 feet over the equator (i.e. it is not uniform). It is very important in aviation because weather happens here. It is characterized by decreasing temperature at a rate of about 2 degrees C for every thousand feet of altitude until it reaches a low of about -55 degrees C. At the top is a thin layer called the Tropopause which traps water vapour in the lower level. The Stratosphere extends upward from the tropopause about 22 miles. It is characterized by a constant temperature of – 55 degrees C and no moisture (water vapour).
Pressure Changes with Altitude

The atmosphere has weight and exerts pressure on the earth and every object it surrounds. It is expressed in several ways such as 14.7 lbs/square inch or 29.92”Hg (inches of mercury) at sea level. As we ascend this pressure drops such that:
This phenomenon is of critical importance in aviation physiology as you will see. The atmosphere is made up of a mixture of gases in constant motion. Nitrogen (78%) and Oxygen (21%) are the most abundant gases, with much smaller percentages of other gases, including Carbon Dioxide. Understand that, although the percentages of the gases remain constant with altitude, their absolute quantity diminishes as one ascends (i.e. there are fewer molecules per unit of volume). This is due to the decrease in pressure with altitude.
- AT SEA LEVEL THE PRESSURE IS 29.92”Hg
- AT 18000’ THE PRESSURE IS HALF OR 14.96”Hg
- AT 33,700’ THE PRESSURE IS HALF AGAIN OR 7.48”Hg
This phenomenon is of critical importance in aviation physiology as you will see. The atmosphere is made up of a mixture of gases in constant motion. Nitrogen (78%) and Oxygen (21%) are the most abundant gases, with much smaller percentages of other gases, including Carbon Dioxide. Understand that, although the percentages of the gases remain constant with altitude, their absolute quantity diminishes as one ascends (i.e. there are fewer molecules per unit of volume). This is due to the decrease in pressure with altitude.
Barometric Pressure
For those mathematically inclined who like formulae, the laws below describe the effects of decreased barometric pressure and how it interplays with the human body. They provide a mathematical description of the phenomena as well as a method to predict what conditions will exist under specific circumstances. For our purposes the formulae are not important--but the concepts they describe are.
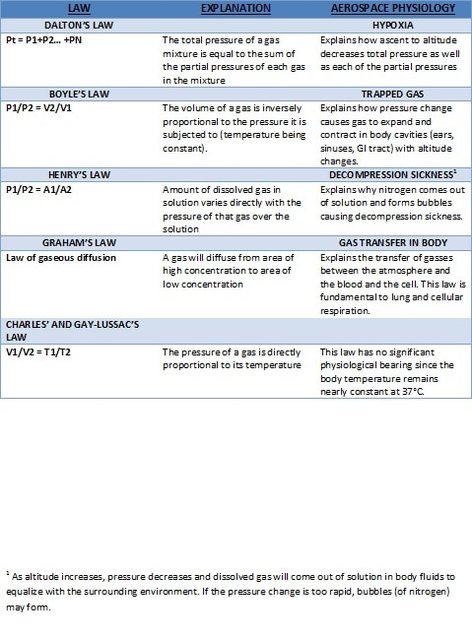
In subsequent installments we will focus on exactly how these laws result in physiologic problems during flight and how to prevent or mitigate them.
The next blog will be a brief discussion on hypoxia, particularly altitude hypoxia.
The next blog will be a brief discussion on hypoxia, particularly altitude hypoxia.










 RSS Feed
RSS Feed